Damage to the Liver Which Can Result From Heavy Alcohol Consumption Is Known as

Introduction
Although heavy drinking can cause a bully deal of health damage ranging from cirrhosis of the liver to pancreatitis, horror stories of alcoholic brain damage are largely a myth. Although wet encephalon is existent, it can exist prevented by proper nutrition and is not directly caused by booze itself.
Booze, Brain Cells, and Encephalon Shrinkage
It has long been an established fact that actively drinking, alcohol dependent subjects accept smaller brain volumes than normal control subjects who exercise not drink alcohol. Early on researchers assumed that this was considering alcohol killed the brain cells of alcohol dependent subjects, only current enquiry proves that this hypothesis is largely untrue. Unless there has been brain damage every bit a result of liver failure or thiamine deficiency, the majority of brain cells of heavy drinkers are intact fifty-fifty though the encephalon has shrunk. We have also discovered that a long period of abstinence or moderate drinking tends to restore the book of heavy drinker'south brains back to normal.
The homo encephalon consists of white cells and gray cells. The gray cells are responsible for thinking and feeling and decisions--they correspond to the Central Processing Unit of measurement (CPU) of your computer. The white cells are similar the cables of your computer which connect the keyboard and the monitor to the CPU. In 1993 Jensen and Pakkenberg did brain cell counts which compared the number of cells in the brains of heavy drinkers with those of nondrinkers. What they constitute was that the number of grey cells was the same in both the heavy drinkers and the nondrinkers. Withal, there were fewer white brain cells in the brains of the drinkers which implies that alcohol kills white brain cells.
In 2009 George Fein discovered that there was one role of the brain in the parietal lobe--which is associated with spatial processing--where booze kills greyness cells. Fein claims that this explains why even subsequently alcohol dependent subjects regain utilise of all their other cerebral functions they still seem to have difficulties with spatial processing.
Studies by Pfefferbaum (1995, 1998) show that with long periods of abstinence or moderate drinking the brains of alcoholic dependent subjects return to nigh the same size equally their nondrinking counterparts.
It is not conclusive whether shrinkage is more pronounced in males, in females, or the same in both (Hommer, 2003).
To summarize: The brains of long term, heavy drinkers shrink, simply they render to almost total normal size after a long menstruation of abstinence or moderate drinking. Long-term, heavy drinking kills some white brain cells and some of the gray cells responsible for spatial processing; yet, it does not kill whatever other greyness cells. In item, the grayness cells which are responsible for our thinking, conclusion making, and other cognitive processes remain intact fifty-fifty in long-term, heavy drinkers. Unless in that location is brain damage which is due to thiamine deficiency or liver failure about all brain functions of booze dependent drinkers tin can be returned to normal with a long flow of abstinence or moderate drinking. Cognitive functioning tends to return to normal when brain size returns to normal.
There is some evidence that both the amount of encephalon shrinkage and the corporeality of cognitive deficit are dependent on the quantity of alcohol consumed and the number of years of heavy drinking; information technology is not established whether this relationship is linear or not.
Amnesia and Dementia Due To Thiamine Deficiency - Wernicke-Korsakoff Syndrome Aka Moisture Brain
The condition known every bit wet encephalon or Wernicke-Korsakoff Syndrome is a class of brain harm which is characterized by astringent amnesia, confabulation, and sometimes dementia (Emsley, et al. 1996). It is non caused by direct furnishings of booze on the encephalon. It is caused by a astringent deficiency of Thiamine (vitamin B1) and is oftentimes precipitated by a sudden influx of glucose. A number of things have been shown to lead to a severe enough thiamine deficiency to trigger wetbrain. These include a nutrition consisting solely of polished rice, prolonged bouts of morning sickness, bulimia and severe alcohol dependence.
Wetbrain has a sudden onset--it is non something which happens gradually over time. The first stage of wetbrain is called Wernicke'southward encephalopathy. When there is a sudden influx of glucose in a brain which is deprived of thiamine the brain cells brainstorm to dice. This is considering the chemical reactions which supply these brain cells with energy for life employ thiamine to plow glucose into free energy in a chemical process called the Krebs cycle. When at that place is an influx of glucose and no thiamine to help metabolize it, these brain cells burn out like a auto engine running on high octane gasoline at high speed with no oil. The brain cells which die first are the ones which crave the most thiamine to function. These brain cells are located around the centre of the brain and are the brain cells which are associated with retention and muscular motion. The brain cells of the cerebellum, which controls balance, are besides affected.
The symptoms of Wernicke's encephalopathy are confusion, lack of coordination, and involuntary heart movements. If Wernicke's encephalopathy is immediately treated with thiamine it tin be stopped and largely reversed. However, if Wernicke'south encephalopathy is not immediately treated, it speedily turns into Korsakoff's psychosis, which is permanent and largely resistant to handling. Symptoms of Korsakoff's syndrome include loss of past memories, inability to acquire new things, confabulation (remembering things which never happened), lack of coordination and unsteady gait, and in severe cases dementia. In some cases physicians who should take known better take precipitated Wernicke-Korsakoff syndrome in patients by putting them on a glucose baste instead of a thiamine drip.
Alcohol tends to block absorption of thiamine by the human torso, so all people who drinkable alcohol should be careful to eat well and should also take vitamin B1 pills to make sure that they are getting plenty thiamine. Severely heavy drinkers who consume around a fifth or a quart of vodka per twenty-four hours are oft also nauseous too nauseous to eat well and may tend to vomit up what they do eat. Moreover, if these people are living on the streets, they may be unwilling to spend money on food which could be used to buy alcohol. These people are in the greatest danger of developing Wernicke-Korsakoff syndrome.
Breedlove (2007) tells us that all cases of wetbrain due to alcohol ingestion could exist prevented by regulations requiring that thiamine exist added to alcoholic beverages. It is unfortunate that our puritanical US society prefers to send people to abstinence-based programs which fail rather than to eliminate much human being suffering past implementing the uncomplicated harm reduction policy of adding thiamine to alcoholic beverages.
HAMS recommends that all drinkers be sure to consume nutritious meals and take vitamins--especially thiamine--to assistance ward off wetbrain. It is also good to effort and take some abstinence days or otherwise reduce booze intake to assistance forbid this.
Wetbrain is sometimes complicated by hepatic encephalopathy.
Hepatic Encephalopathy
Hepatic encephalopathy is damage to the brain which is a result of liver failure, which may be caused by cirrhosis, hepatitis, etc. One job of the liver is to screen out toxins and so that they can exist disposed of as waste material rather than circulate in the claret and damage delicate tissues like the brain. When the liver fails information technology is believed that toxins similar ammonia and manganese cross the claret-brain bulwark and cause damage to the brain--i. due east. hepatic encephalopathy.
Symptoms of hepatic encephalopathy include sluggishness, apathy, disorientation, inappropriate behavior, and slurred speech. In severe cases there may be blackout.
If alcohol causes liver failure so hepatic encephalopathy tin be 1 effect.
Alcohol and Cognitive Dysfunction
People who drink massive quantities of booze endure brain shrinkage and cognitive dysfunction as a result. Nevertheless, the expert news is that if these heavy drinkers do not have thiamine-related brain damage or liver-related encephalon damage and then this cognitive dysfunction and brain shrinkage is almost entirely reversible with a change from heavy drinking to reduced drinking or alcohol forbearance.
Although well-nigh researchers emphasize alcohol abstinence, research from Sullivan et al (2000b) demonstrates that reduced drinking also restores cognitive function in formerly alcohol dependent drinkers: abstinence is not the only solution
The information in Table 1 is a conflation of information independent in 2 papers by George Fein virtually recovery of cerebral function later on stopping heavy drinking. One paper is a literature review published in 1990 and the other is a written report published in 2006.
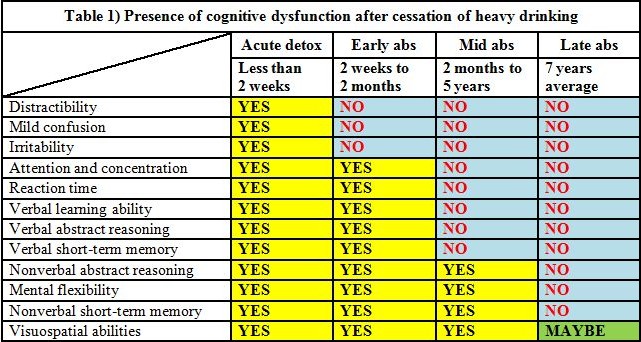
Although Fein's 1990 paper gives a spread of two months to five years for mid phase recovery of cognitive function, Fein's 2006 paper narrows this downward and tells us that that these cognitive functions are generally recovered at the finish of the first year after ceasing heavy drinking. Parsons (1998) states that remission of cerebral dysfunction occurs at 4 to 5 years.
In Fein's 2006 study the male person drinkers at their pinnacle drinking consumed 361.8 ± 257.ii standard drinks per month for a menses of 51.0 ± 30.9 months. The female person drinkers at their peak consumed 264.0 ± 202.viii standard drinks per month for a menstruum of 92.1 ± 81.ii months. (Ane standard drink = 14g ETOH.) This is around a half a liter of vodka (80 proof) per day every day for the men and effectually a "pint" (375 ml) of vodka per day every 24-hour interval for the women. Control subjects averaged less than one-half a potable per twenty-four hours.
According to Parsons 1998 there is no significant deference between alcohol dependent males and females on the variable of cognitive dysfunction.
Although the dose, the frequency, and the elapsing of alcohol consumption all announced to have an effect on the caste of cognitive dysfunction (as well every bit degree of incoordination) the human relationship is non entirely clear cut. Parsons (1998) proposes a nonlinear, tripartite, threshold model of the effect of alcohol dose on cognitive dysfunction every bit exemplified in Tabular array 2.
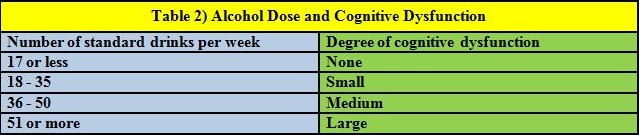
(Annotation: In their original paper Parson and Nixon used the old definition of a US standard drink--12g ETOH. This has been corrected to the current 14g definition here.)
Sullivan (2000c) tells the states that calorie-free relapsers performed comparably to abstinent subjects on cognitive tests at the mid stage catamenia of recovery of cerebral function which suggests that reduced drinking may be as expert a strategy as forbearance for the recovery of cognitive role in formerly dependent drinkers.
We should also note that these cognitive deficits are present statistically--when nosotros look at actual individuals there are some alcohol dependent subjects in acute detox stage who show improve cognitive role than some normal controls--information technology is just that they are a small minority. Parsons (1998) plant 85% discrimination between the control grouping and the alcohol dependent group when the ways of several tests were taken into business relationship. This means that xv% of the alcohol dependent subjects were showing cognitive performance equal to that of the controls.
In summary: Heavy drinkers who consume around a quart of booze or so every day suffer from cognitive defects and brain shrinkage. When these heavy drinkers quit drinking or reduce their consumption of alcohol to reasonable levels nigh of these cognitive dysfunction and much of this brain shrinkage goes away by the finish of the outset year. Near all of the cognitive dysfunction and brain shrinkage is gone at the at the end of 5 or so years except for some loss of white affair, a small loss of grey affair which controls spatial processing, and some minor dysfunction of spatial processing in some individuals. This is true for heavy drinkers who do non have thiamine related encephalon damage or encephalon impairment related to liver failure which are permanent.
Conclusion
We should have learned long ago that scare tactics based on lies non only neglect, but backfire and lead to worse issues than earlier. When kids found that "Reefer Madness" was a prevarication they stopped believing warnings about heroin, too. Since nosotros know that drunkards like Hemingway, O'Neill, Faulkner and Steinbeck managed to win the Nobel Prize in Literature in spite of their drinking habits this puts a prevarication to the myth that every drinker turns into a brain damaged idiot. The time to put an terminate to the lies is now. Drinking a fifth of liquor a 24-hour interval is conspicuously not good for your health, just if you sentinel your nutrition and continue a handle on things then occasionally engaging in recreational intoxication is non nearly so bad as the fear-mongers would lead us to believe.
Lying to kids by telling them that a single night of heavy drinking will turn their brain into a walnut is irresponsible. Kids observe adults engaging in occasional recreational intoxications without suffering major brain harm and they know that they are beingness lied to. One time you lie to kids y'all lose your credibility for good because kids are existent black and white thinkers. Once you have cried wolf and then kids will non believe yous when yous warn them about existent dangers like drinking and driving, the addictive nature of heroin, or the fact that drinking a fifth of liquor a day tin rot your liver.
Permit'south stop all the scare tactics and tell kids the truth for a modify--okay?
The life yous salve may exist your kid'southward.
REFERENCES:
Breedlove SM, Rosenzweig MR, Watson NV. (2007). Biological Psychology: An Introduction to Behavioral, Cerebral, and Clinical Neuroscience. Fifth Edition. Sinauer Assembly, Inc.
Dlugos, CA and Pentney, RJ. (1997). Morphometric evidence that the total number of synapses on Purkinje neurons of one-time F344 rats is reduced later on long-term ethanol handling and restored to control levels later on recovery. Alcohol and alcoholism (Oxford, Oxfordshire) 32 (2), 161-72
PubMed Abstruse: http://www.ncbi.nlm.nih.gov/pubmed/9105510
PMID:9105510
Free Full Text: http://alcalc.oxfordjournals.org/content/alcalc/32/2/161.total.pdf
Emsley, R. et al. (1996). Magnetic resonance imaging in alcoholic Korsakoff's syndrome: evidence for an association with alcoholic dementia. Alcohol and alcoholism (Oxford, Oxfordshire) 31 (5), 479-86
PubMed Abstract: http://world wide web.ncbi.nlm.nih.gov/pubmed/8949964
PMID:8949964
Gratuitous Full Text: http://alcalc.oxfordjournals.org/content/alcalc/31/5/479.full.pdf
Fama, R Marsh, Fifty and Sullivan, EV. (2004). Dissociation of remote and anterograde memory damage and neural correlates in alcoholic Korsakoff syndrome. Journal of the International Neuropsychological Society: JINS. 10 (3), 427-41
PubMed Abstract: http://www.ncbi.nlm.nih.gov/pubmed/15147600
PMID:15147600
doi:10.1017/S135561770410310X
Fama, R et al. (2007). Upper and lower limb motor impairments in alcoholism, HIV infection, and their comorbidity. Alcoholism, clinical and experimental research. 31 (6), 1038-44
PubMed Abstruse: http://www.ncbi.nlm.nih.gov/pubmed/17403062
PMID:17403062
doi:ten.1111/j.1530-0277.2007.00385.ten
Fama, R Pfefferbaum, A and Sullivan, EV. (2004). Perceptual learning in detoxified alcoholic men: contributions from explicit memory, executive function, and age. Alcoholism, clinical and experimental research. 28 (11), 1657-65
PubMed Abstruse: http://www.ncbi.nlm.nih.gov/pubmed/15547452
PMID:15547452
Fein, G et al. (2009). Parietal grayness matter volume loss is related to spatial processing deficits in long-term abstinent alcoholic men. Alcoholism, clinical and experimental enquiry. 33 (x), 1806-14
PubMed Abstract: http://www.ncbi.nlm.nih.gov/pubmed/19645730
PMID:19645730
doi:10.1111/j.1530-0277.2009.01019.10
Fein, Thou et al. (2006). Cognitive performance in long-term abstinent alcoholic individuals. Alcoholism, clinical and experimental inquiry. 30 (9), 1538-44
PubMed Abstract: http://www.ncbi.nlm.nih.gov/pubmed/16930216
PMID:16930216
doi:x.1111/j.1530-0277.2006.00185.x
Complimentary Total Text: http://world wide web.ncbi.nlm.nih.gov/pmc/articles/PMC1868685/pdf/nihms20940.pdf
Fein, Yard et al. (1990). Cognitive impairments in abstinent alcoholics. The Western periodical of medicine. 152 (5), 531-vii
PubMed Abstract: http://www.ncbi.nlm.nih.gov/pubmed/2190421
PMID:219042
Complimentary Full Text: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1002406/pdf/westjmed00117-0069.pdf
Harper, C and Kril, J. (1991). If you drink your brain volition shrink. Neuropathological considerations. Alcohol and alcoholism. (Oxford, Oxfordshire). Supplement i, 375-80
PubMed Abstruse: http://www.ncbi.nlm.nih.gov/pubmed/1845566
PMID:1845566
Harper, C and Kril, J. (1994). An introduction to alcohol-induced brain damage and its causes. Booze and alcoholism. (Oxford, Oxfordshire). Supplement 2, 237-43
PubMed Abstract: http://world wide web.ncbi.nlm.nih.gov/pubmed/8974342
PMID:8974342
Hommer, DW. (2003). Male and female person sensitivity to alcohol-induced brain damage. Alcohol research & health : the journal of the National Institute on Alcohol Abuse and Alcoholism. 27 (2), 181-5
PubMed Abstruse: http://www.ncbi.nlm.nih.gov/pubmed/15303629
PMID:15303629
Free Full Text: http://pubs.niaaa.nih.gov/publications/arh27-2/181-185.pdf
Jensen, GB and Pakkenberg, B. (1993). Do alcoholics beverage their neurons abroad? Lancet. 342 (8881), 1201-4
PubMed Abstract: http://world wide web.ncbi.nlm.nih.gov/pubmed/7901529
PMID:7901529
Moselhy, HF Georgiou, K and Kahn A. (2001). Frontal lobe changes in alcoholism: a review of the literature. Booze and alcoholism. (Oxford, Oxfordshire) 36 (5), 357-68
PubMed Abstract: http://www.ncbi.nlm.nih.gov/pubmed/11524299
PMID:11524299
Free Total Text: http://alcalc.oxfordjournals.org/content/alcalc/36/5/357.full.pdf
Oscar-Berman, M and Marinković, Grand. (2007). Alcohol: effects on neurobehavioral functions and the encephalon. Neuropsychology review. 17 (three), 239-57
PubMed Abstruse: http://www.ncbi.nlm.nih.gov/pubmed/17874302
PMID:17874302
doi:10.1007/s11065-007-9038-six
Oscar-Berman, M et al. (Apr 2004). Comparisons of Korsakoff and not-Korsakoff alcoholics on neuropsychological tests of prefrontal brain performance. Alcoholism, clinical and experimental inquiry. 28 (four), 667-75
PubMed Abstract: http://www.ncbi.nlm.nih.gov/pubmed/15100620
PMID:15100620
Parsons, OA. (1998). Neurocognitive deficits in alcoholics and social drinkers: a continuum? Alcoholism, clinical and experimental research. 22 (4), 954-61
PubMed Abstract: http://www.ncbi.nlm.nih.gov/pubmed/9660328
PMID:9660328
Parsons, OA and Nixon, SJ. (1998). Cognitive functioning in sober social drinkers: a review of the research since 1986. Journal of studies on alcohol. 59 (two), 180-ninety
PubMed Abstruse: http://www.ncbi.nlm.nih.gov/pubmed/9500305
PMID:9500305
Pfefferbaum, A et al. (October 1995). Longitudinal changes in magnetic resonance imaging brain volumes in abstinent and relapsed alcoholics. Alcoholism, clinical and experimental research. nineteen (v), 1177-91
PubMed Abstruse: http://www.ncbi.nlm.nih.gov/pubmed/8561288
PMID:8561288
Pfefferbaum, A et al. (1998). A controlled study of cortical grey matter and ventricular changes in alcoholic men over a 5-yr interval. Archives of general psychiatry. 55 (ten), 905-12
PubMed Abstract: http://world wide web.ncbi.nlm.nih.gov/pubmed/9783561
PMID:9783561
Salen, PN. Wernicke Encephalopathy. eMedicine.
http://emedicine.medscape.com/article/794583-overview
Accessed October 29, 2009.
Sullivan, EV and Marsh, L. (2003). Hippocampal volume deficits in alcoholic Korsakoff'southward syndrome. Neurology. 61 (12), 1716-9
PubMed Abstract: http://world wide web.ncbi.nlm.nih.gov/pubmed/14694035
PMID:14694035
Sullivan, EV et al. (2000). Cerebellar volume decline in normal aging, alcoholism, and Korsakoff's syndrome: relation to clutter. Neuropsychology. 14 (3), 341-52
PubMed Abstract: http://www.ncbi.nlm.nih.gov/pubmed/10928737
PMID:10928737
Sullivan, EV Rosenbloom, MJ and Pfefferbaum. A. (2000). Pattern of motor and cognitive deficits in detoxified alcoholic men. Alcoholism, clinical and experimental inquiry. 24 (5), 611-21
PubMed Abstract: http://www.ncbi.nlm.nih.gov/pubmed/10832902
PMID:10832902
Sullivan, EV et al. (2000). Longitudinal changes in knowledge, gait, and balance in abstinent and relapsed alcoholic men: relationships to changes in encephalon construction. Neuropsychology. 14 (two), 178-88
PubMed Abstract: http://www.ncbi.nlm.nih.gov/pubmed/10791858
PMID:10791858
Sullivan, EV et al. (2002). Speed and efficiency but not accuracy or timing deficits of limb movements in alcoholic men and women. Alcoholism, clinical and experimental research. 26 (v), 705-13
PubMed Abstract: http://www.ncbi.nlm.nih.gov/pubmed/12045480
PMID:12045480
Sullivan, EV et al. (2002). A profile of neuropsychological deficits in alcoholic women. Neuropsychology. xvi (ane), 74-83
PubMed Abstract: http://world wide web.ncbi.nlm.nih.gov/pubmed/11853359
PMID:11853359
Wolf, DC. Encephalopathy, Hepatic. eMedicine.
http://emedicine.medscape.com/article/186101-overview
Accessed October 29, 2009.
Xiong, GL. Wernicke-Korsakoff Syndrome. eMedicine.
http://emedicine.medscape.com/commodity/288379-overview
Accessed October 29, 2009.
Source: https://hams.cc/brain_damage/
0 Response to "Damage to the Liver Which Can Result From Heavy Alcohol Consumption Is Known as"
Post a Comment